

Abstract
Introduction: Cancer patients tend to have a higher incidence of venous thromboembolism (VTE) - pulmonary embolism (PE) and deep venous thrombosis (DVT). There is conflicting data in the literature about the incidence of VTE in solid tumors versus hematological cancers. The purpose of this study was to analyze the prevalence of PE, DVT, and VTE in hospitalized patients with solid and hematologic malignancies using the National Inpatient Sample database.
Methods: We performed a retrospective cohort analysis of the National Inpatient Sample 2014 Database (HCUP-NIS). Patients were included in the study if they had a principal diagnosis of DVT, PE, or both (VTE); primary or secondary diagnosis of solid tumors or hematological malignancy; and age 18 years or older. We performed univariate and multivariate regression to analyze the association of PE, DVT, and VTE with solid versus hematologic cancers. We performed univariate and multivariate regression to determine their statistical significance. We also performed univariate analysis for tumor type and saddle PE and upper extremity DVT. All analyses applied the HCUP-NIS weights.
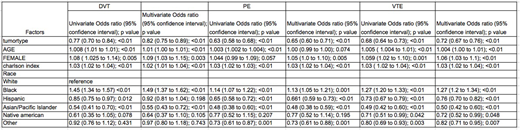
Results: We identified 27,410 patients with isolated DVT; 41,645 with isolated PE; and 69,055 with both DVT and PE (VTE). On multivariate analysis, hematologic malignancy had lower odds of DVT (OR 0.82, 95% CI 0.75-0.89), isolated PE (OR 0.65, 95% CI 0.60 - 0.71) and VTE (OR 0.72, 95% CI 0.67-0.76). Female sex and Charlson index were associated with modest increased odds of DVT, PE and VTE (OR <1.10 for all), while Asian/Pacific Islander race was associated with lower odds for each (OR 0.48-0.55). In contrast, black race was associated with greater odds of DVT (OR 1.49, 95% CI 1.37-1.62) and VTE (OR 1.27, 95% CI 1.2-1.34), but lower odds of isolated PE (OR 0.48, 95% CI 0.38-0.59). Native American and other race had lower odds of VTE (OR 1.27, 95% CI 1.2-1.34 and OR 0.82, 95% CI 0.71-0.95, respectively). Hispanic ethnicity had lower odds of PE (OR 0.66, 95% CI 0.59-0.73) and VTE (OR 0.76, 95% CI 0.70-0.82). Although, 91.1% of patients with malignancy and saddle PE had solid tumors, tumor type (solid versus hematological) was not statistically significant on univariate regression analysis (OR 0.83, 95% CI 0.58-1.18). Hematologic malignancy was associated with less upper extremity DVT (OR 0.69, 95% CI 0.54-0.88).
Discussion: Based on the above data, patients with solid tumors are more likely to develop isolated DVT, PE, VTE, and upper extremity DVT. The analysis was likely underpowered to identify a difference for saddle PE, a relatively rare event with high mortality. Race appears to be associated in complex ways. In particular, it is unclear why black patients have increased odds of developing DVT or VTE, but lower odds for isolated PE. Two possible explanations are differences in health seeking behavior or increased outpatient mortality for isolated PE. As with saddle PE, it's likely the sample was too small to find differences for isolated DVT or PE for Native Americans and others. Additional studies to examine the reasons for differences by tumor type and race/ethnicity are needed.
Bussel:Rigel: Consultancy, Research Funding; Amgen Inc.: Consultancy, Research Funding; Protalex: Consultancy; Novartis: Consultancy, Research Funding; Momenta: Consultancy; Uptodate: Honoraria; Prophylix: Consultancy, Research Funding. Marks:Seattle Genetics: Equity Ownership; Heron: Membership on an entity's Board of Directors or advisory committees; Lilly: Membership on an entity's Board of Directors or advisory committees; Odonate: Membership on an entity's Board of Directors or advisory committees; UPMC: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal